
Newborn Fall Prevention and Reduction: A QI Roadmap
To support the inclusion of Newborn Falls within Quality Assurance and Performance Improvement (QAPI) efforts, here is a start for your teams to “plug in” a QI framework that addresses preventing and reducing newborn falls during the immediate postpartum stay.
Posted under: Quality of Care
What do you notice in hospitals and units where QI works well and results are sustainable over time? You will notice a commitment to QI from the Board to the frontline to patients and a shared mental model of the necessary components to support newborn patient safety.
When the National Perinatal Information Center released its Newborn Falls and Drops webinar, we were gratified to experience a deluge of interest and completions. Even with the most recent update Newborn Falls: An Interactive Discussion to Achieve Best Practices, we continue experiencing that increasing interest volume. This tells us something: Newborn Falls is an area of interest but rarely included within yearly education and Quality Improvement (QI) teams and/or projects.
To support the inclusion of Newborn Falls within Quality Assurance and Performance Improvement (QAPI) efforts, here is a start for your teams to “plug in” a QI framework that addresses preventing and reducing newborn falls during the immediate postpartum stay.
Quality Improvement is not simply a “one-and-done” process. QI is an iterative process requiring a continual planning, assessment, and evaluation cycle.
Overarching Best Practices for Newborn Quality Improvement Initiatives
Hospital Leadership/Boards of Directors
Nursing and Physician Leadership/Unit Level
Frontline Care Teams
Let's explore your teams themselves and the team members who will be doing the work.
Believe it or not, naysayers are not only helpful, but can be very valuable to identifying barriers and real/potential pitfalls of a QI project. The "squeaky wheels" can be some of your most invested team members who sincerely want positive change. Or they have had enough of “one trick ponies” and QI projects that were not sustainable or implemented without frontline feedback. While it may be tempting to dismiss them, it is much more important to listen and hear their concerns.
And diving EVEN further, assuming everything is lining up…
The Patients Themselves.
Earlier I mentioned the engagement of patients in QI project development. Yes, this is a critical component of successful QI implementation. As important as it is for your organization and team to be engaged and dedicated to QI, what if the newborn fall reduction project you are considering does not meet the needs of your patients?
Even before exploring buy-in, let’s explore some potentially hidden assumptions about the immediate postpartum period and newborn fall prevention/reduction:
Hospital Leadership:
Social Drivers of Health
A Social Drivers of Health (SDoH) evaluation is essential to address at admission to both Labor and Delivery and the Postpartum unit.
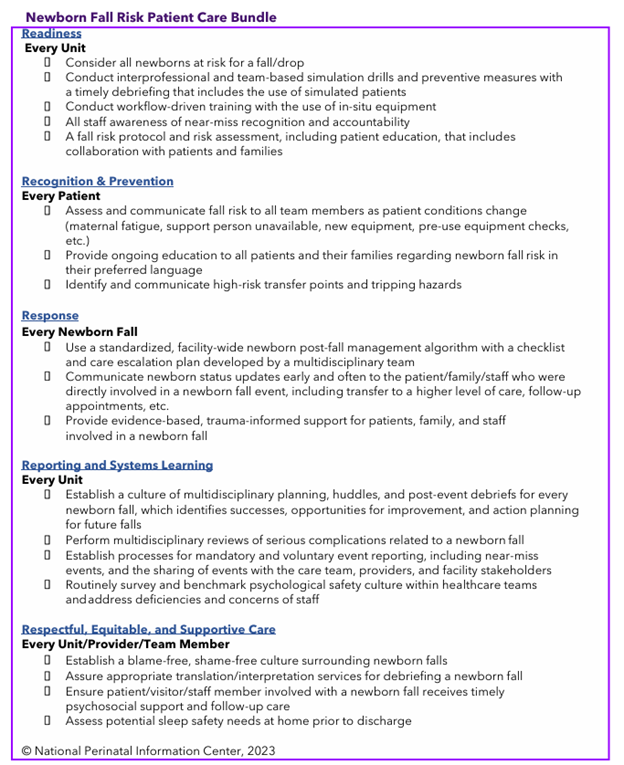
Successful QI implementation takes organizational commitment, time, and supportive leadership. Using this QI framework to prevent and reduce newborn falls in conjunction with the Newborn Fall Patient Safety Bundle may support your efforts to enhance patient safety and create meaningful conversations between your patients and care teams.
Need assistance in creating and implementing your Newborn Fall Quality Improvement project? Reach out to NPIC for more information.
When the National Perinatal Information Center released its Newborn Falls and Drops webinar, we were gratified to experience a deluge of interest and completions. Even with the most recent update Newborn Falls: An Interactive Discussion to Achieve Best Practices, we continue experiencing that increasing interest volume. This tells us something: Newborn Falls is an area of interest but rarely included within yearly education and Quality Improvement (QI) teams and/or projects.
To support the inclusion of Newborn Falls within Quality Assurance and Performance Improvement (QAPI) efforts, here is a start for your teams to “plug in” a QI framework that addresses preventing and reducing newborn falls during the immediate postpartum stay.
Quality Improvement is not simply a “one-and-done” process. QI is an iterative process requiring a continual planning, assessment, and evaluation cycle.
Overarching Best Practices for Newborn Quality Improvement Initiatives
Hospital Leadership/Boards of Directors
- Is hospital leadership (yes, I mean the Board of Directors and the C-Suite) invested in elevating newborn care?
- Are neonatal health and outcome disparities on the agenda of Boards of Directors/Trustee meetings? How often?
- Do Boards of Directors/Trustees/C-Suite ask about QI projects on a routine basis?
- Do they routinely ask about outcome disparities?
- How often do they see QI data? And is this data shared with Boards of Directors? Trustees?
- How engaged is the Board in reviewing and understanding neonatal (both well and sick newborn) QI projects?
- Do unit leaders have an opportunity to engage directly with the Board and share best practices and success stories of improved neonatal and newborn care, particularly through a racial and ethnic lens?
Nursing and Physician Leadership/Unit Level
- What does nursing leadership look like? Invested in QI? Or is it just another “check the box” exercise?
- What does physician/provider leadership look like? Invested in QI?
- Does nursing and physician leadership work well together? Solid leadership dyad?
- Are they committed to the same outcomes and priorities?
- Are they committed to including the voices of those most impacted in neonatal and newborn project planning?
- In other words, are patients of color or others based upon identified social needs asked to participate in QI initiatives within the unit?
- Is there a Patient Advisory Council that facilitates connections between patients and care teams? Is this viewed as a strength by the nursing/physician leadership dyad?
- Have they assessed the activation and readiness of their teams to engage in QI work?
Frontline Care Teams
Let's explore your teams themselves and the team members who will be doing the work.
- Are they ready to engage in QI work?
- Are postpartum doulas (yes, you read that right…POSTPARTUM DOULAS) considered part of the frontline care team related to newborn fall prevention and reduction?
- Did the frontline care team have input in creating the QI project?
- Are there identified champions and informal leaders?
- Is there bandwidth available?
- How many other projects and initiatives are underway?
- Is this considered a priority among many others? Could your frontline teams identify the quality improvement priorities in your unit/department?
- Is the team multidisciplinary and includes all facets of care?
- Are there identified naysayers?
Believe it or not, naysayers are not only helpful, but can be very valuable to identifying barriers and real/potential pitfalls of a QI project. The "squeaky wheels" can be some of your most invested team members who sincerely want positive change. Or they have had enough of “one trick ponies” and QI projects that were not sustainable or implemented without frontline feedback. While it may be tempting to dismiss them, it is much more important to listen and hear their concerns.
And diving EVEN further, assuming everything is lining up…
The Patients Themselves.
Earlier I mentioned the engagement of patients in QI project development. Yes, this is a critical component of successful QI implementation. As important as it is for your organization and team to be engaged and dedicated to QI, what if the newborn fall reduction project you are considering does not meet the needs of your patients?
- Were assumptions made based upon conscious/unconscious bias rather than data?
- Are the measures/objectives/metrics aligned with the communities you serve?
- How will patients react to and participate in a QI initiative? Are they passive or active participants?
Even before exploring buy-in, let’s explore some potentially hidden assumptions about the immediate postpartum period and newborn fall prevention/reduction:
- Are patients expected to be awake all night? And all day? How are a patient’s sleep needs addressed within your Postpartum care policies?
- Do your Perinatal teams understand the importance of maternal sleep science within the immediate postpartum period?
- What type of newborn fall education is provided to patients? Do you rely on a “care contract” to prevent newborn falls?
- Has your facility defined what a “near miss” is related to a newborn fall? Are near misses measured and reported? Or only the actual fall?
- What type of newborn fall risk assessment is completed? How often? Is it evidence-based?
- Are care team members beyond RNs included in newborn fall prevention? This includes certified nursing assistants (CNAs), unit clerks, and other key ancillary team members.
- What change models are used in your organization? (And yes, there is a process to cultivating change).
Hospital Leadership:
- Awareness of newborn falls in the last month/year?
- View newborn falls as an identified patient safety risk?
- Frequency and evaluation of newborn falls and any disparities that exist?
- Rounding on units to assess for engagement in newborn fall prevention and reduction? Barriers to implementation?
- Agreement on the importance of newborn fall prevention and reduction efforts?
- Mutual support from RN/MD leadership?
- Awareness and involvement of all team members to support the initiative, including other care team members involved in care? And yes, this includes Environmental Services, Case Management, Food and Nutrition Services, Biomedical Engineering, Pharmacy, Respiratory Therapy, and anyone meeting a patient. Does everyone buy into the importance of patient safety and newborn fall prevention?
- Students part of the process and encouraged to participate in and lead QI activities?
- Does your frontline care team look like the patients you are serving? If not, what steps has your organization taken to diversify your team to ensure newborn fall education is meeting the needs of your patients?
- How are postpartum doulas utilized in the prevention of newborn falls?
- Ongoing education? Is it Just-in-Time/bite size for ease of use?
- Use of preferred language materials to promote real-time education for patients?
- How are QI Champions supported? Dedicated time for support of the QI project?
- Understanding and appreciating the importance of evidence-based practice?
- How are newborn fall prevention QI activities incorporated into daily processes? How are they communicated to teams? How do teams communicate initiatives and outcomes to each other?
- Have they been heard? Have their concerns been addressed? Even if unable to meet the need, has the inability to provide (XXX) been discussed?
- Have QI projects become “one more thing” to do? How has that perception been addressed?
- Are there competing priorities that have not been addressed? How are QI projects and other organizational needs prioritized? Communicated to teams?
- Are there sufficient resources to support newborn fall prevention in the unit?
- Have any personal conscious/unconscious racial biases been addressed that may be creating negativity towards equity work?
- Have diverse patients been included in providing feedback related to their postpartum care and education experience?
- Has the newborn falls prevention QI project been introduced to patients with feedback elicited before implementation?
- Is a Patient Advisory Committee or Team included in the QI project and process for enhancing newborn fall prevention?
- Have patients been asked about resources, supplies, and other needs related to newborn fall reduction?
- Is your patient insisting on co-sleeping with the baby during the immediate postpartum stay? Has this been explored through a social driver lens instead of immediately quoting policies and best practices?
Social Drivers of Health
A Social Drivers of Health (SDoH) evaluation is essential to address at admission to both Labor and Delivery and the Postpartum unit.
- Is the patient alone? Who supports the patient during the night between feedings and other newborn care needs?
- Does the patient feel safe in their home? Neighborhood? Environment? Do threats of personal safety impact sleep quality and quantity?
Successful QI implementation takes organizational commitment, time, and supportive leadership. Using this QI framework to prevent and reduce newborn falls in conjunction with the Newborn Fall Patient Safety Bundle may support your efforts to enhance patient safety and create meaningful conversations between your patients and care teams.
Need assistance in creating and implementing your Newborn Fall Quality Improvement project? Reach out to NPIC for more information.