
Creating Quality Improvement New Year Resolutions: Maternal and Newborn Care
Are you among the hospitals who are seeking to improve quality? Have you explored the Psychology of Quality Improvement?
Posted under: Maternal Health, Quality of Care
Hospitals across the country are looking forward to 2024 and sharing the vision of their strategic plans. If you are among the hospitals who are seeking to improve quality, have you explored the Psychology of Quality Improvement?
Last week, I joined others from across the United States at the National Institute for Children’s Health Quality (NICHQ) National Network of Perinatal Quality Collaboratives Annual Meeting. Rhode Island is fortunate to be one of many states funded to support its perinatal quality collaborative.
Many topics were consistently mentioned and I wanted to bring awareness to one of those topics here. Postpartum readmissions were one of the issues being addressed, and how we can continue to bring awareness to the key drivers of readmission.
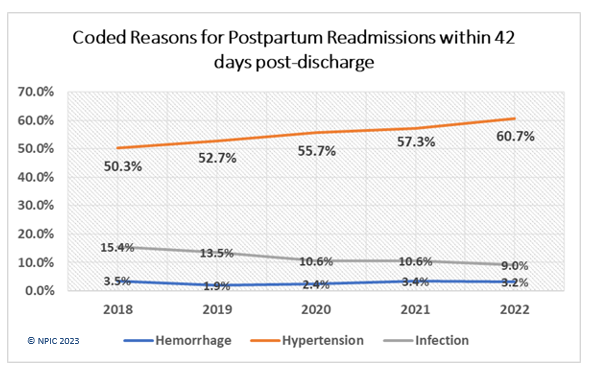
According to the National Perinatal Information Center, between 2018 – 2022, the most frequently reported diagnosis related to postpartum readmission is preeclampsia. Severe hypertension and preeclampsia have continued to rise over the past five years, and that trend does not seem to be changing. Fortunately, there have been great strides in reductions in readmission due to infection, and postpartum hemorrhage has been relatively stable over the past five years.
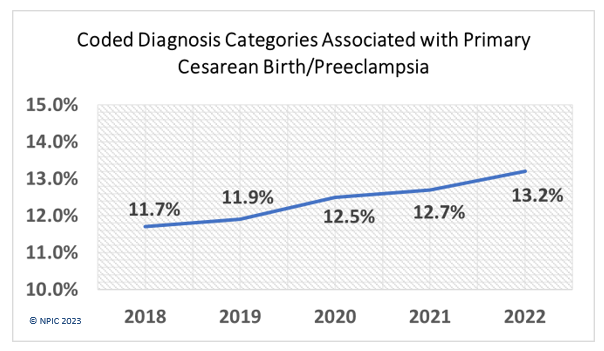
Preeclampsia is not only the driver for postpartum readmission, but it has been a driver for cesarean birth as well. During the years 2018 – 2022, the NPIC Perinatal Database follows coded reasons for cesarean birth, and preeclampsia has had the highest increase over this same five year period.
Many hospitals are seeking resources to impact the rate of preeclampsia and hypertension that are being seen in obstetric units. Maternal morbidity and mortality discussions and review committees (MMRCs) continue to review maternal deaths associated with preeclampsia/severe hypertension/stroke and have finally begun to explore the impact that racism may have had in diagnosing/addressing/treating/responding to hypertension in Black women.
One of the most critical areas addressed during the NNPQC meeting was the Psychology of Quality Improvement. Yes, there is a foundational approach to QI projects that cannot be overstated. Dr. Veronica Gillespie-Bell (Louisiana) provided an outstanding primer on Creating Change and Managing Resistance (yes, managing the resistance to change). There are those who will embrace change. And there are those who will resist change. But there is a way ahead. And here are the secrets:
**normalization of deviance can completely derail change management**
It is very important to address normalization of deviance (NoD) within change management. NoD has been mentioned several times in these blogs over the past year. If you need a refresher, check out our previous discussions. Become familiar with the term. There are reasons that, on average, it takes 17 years to translate research to practice. This is one of them.
Are your frontline teams drivers or mere passengers in the quality improvement process? How can you leverage the bench strength of your teams to effectively create changes in patient care? If your frontline teams do not have an active role in your quality improvement initiatives, you are missing a critical voice in successful (and sustainable!!) change.
It is important to include your patients and families in your quality improvement initiatives, particularly if the target population is patients. Let’s use maternal severe hypertension for a moment.
No matter your priority for this next year, whether it is maternal hypertension, postpartum hemorrhage, safely reducing primary cesarean birth, sepsis, maternal mental health, or other healthcare needs, creating a strategy to implement change in practice or process can take time. But let’s face it…our patients don’t have 17 years to implement change. They are relying on us now to provide the highest quality of evidence-based care.
As part of your New Year resolutions, think about adding sustainable change to your strategy. Change and sustainable change are two different concepts. Quality and patient safety are at or near the top of many hospitals’ strategic plans in 2024 and beyond, with many including high reliability as a metric of success. Achieving these goals are possible, but only with the cumulative efforts of data, knowledge, commitment to equity, and action. And yes, the psychology of quality improvement.
Here's to sustainable change and outstanding quality improvement in 2024. Happy New Year
If your team would like to incorporate sustainable quality improvement in your organization, NPIC can support your strategy. Reach out to us to learn more.
Last week, I joined others from across the United States at the National Institute for Children’s Health Quality (NICHQ) National Network of Perinatal Quality Collaboratives Annual Meeting. Rhode Island is fortunate to be one of many states funded to support its perinatal quality collaborative.
Many topics were consistently mentioned and I wanted to bring awareness to one of those topics here. Postpartum readmissions were one of the issues being addressed, and how we can continue to bring awareness to the key drivers of readmission.
According to the National Perinatal Information Center, between 2018 – 2022, the most frequently reported diagnosis related to postpartum readmission is preeclampsia. Severe hypertension and preeclampsia have continued to rise over the past five years, and that trend does not seem to be changing. Fortunately, there have been great strides in reductions in readmission due to infection, and postpartum hemorrhage has been relatively stable over the past five years.
Preeclampsia is not only the driver for postpartum readmission, but it has been a driver for cesarean birth as well. During the years 2018 – 2022, the NPIC Perinatal Database follows coded reasons for cesarean birth, and preeclampsia has had the highest increase over this same five year period.
Many hospitals are seeking resources to impact the rate of preeclampsia and hypertension that are being seen in obstetric units. Maternal morbidity and mortality discussions and review committees (MMRCs) continue to review maternal deaths associated with preeclampsia/severe hypertension/stroke and have finally begun to explore the impact that racism may have had in diagnosing/addressing/treating/responding to hypertension in Black women.
One of the most critical areas addressed during the NNPQC meeting was the Psychology of Quality Improvement. Yes, there is a foundational approach to QI projects that cannot be overstated. Dr. Veronica Gillespie-Bell (Louisiana) provided an outstanding primer on Creating Change and Managing Resistance (yes, managing the resistance to change). There are those who will embrace change. And there are those who will resist change. But there is a way ahead. And here are the secrets:
- Define the change through an effective vision
- Communicating the change
- Building an improvement team(MUST include frontline staff)
- Develop reinforcement strategies
- Assess the climate for change—cultural, commitment, capacity readiness
- Creating culture for change
- Select the model for change
- Understanding and managing resistance
- Celebrate small wins
**normalization of deviance can completely derail change management**
It is very important to address normalization of deviance (NoD) within change management. NoD has been mentioned several times in these blogs over the past year. If you need a refresher, check out our previous discussions. Become familiar with the term. There are reasons that, on average, it takes 17 years to translate research to practice. This is one of them.
Are your frontline teams drivers or mere passengers in the quality improvement process? How can you leverage the bench strength of your teams to effectively create changes in patient care? If your frontline teams do not have an active role in your quality improvement initiatives, you are missing a critical voice in successful (and sustainable!!) change.
- Are they ready to engage in QI work?
- Did the team have any input in creating the QI project?
- Are there identified champions and informal leaders who can contribute a diverse lens to the process?
- Is there bandwidth available?
- How many other projects and initiatives are underway?
- Is this considered a priority among many others? Who is communicating that priority? (“This is something we have been told to do” versus “We have an opportunity to improve patient care and maternal outcomes”)
- Is the team multidisciplinary and includes all facets of care?
It is important to include your patients and families in your quality improvement initiatives, particularly if the target population is patients. Let’s use maternal severe hypertension for a moment.
- Do you have patients with lived experience on your Quality Improvement projects? How are you ensuring that diverse voices are a part of your work?
- Have your patients reviewed your preeclampsia/hypertension discharge materials? Do they understand them? Are they in a language they understand?
- Are you disaggregating your outcomes data by race and ethnicity? Are your time to treatment outcomes similar, or do you have glaring differences in treatment outcomes?
No matter your priority for this next year, whether it is maternal hypertension, postpartum hemorrhage, safely reducing primary cesarean birth, sepsis, maternal mental health, or other healthcare needs, creating a strategy to implement change in practice or process can take time. But let’s face it…our patients don’t have 17 years to implement change. They are relying on us now to provide the highest quality of evidence-based care.
As part of your New Year resolutions, think about adding sustainable change to your strategy. Change and sustainable change are two different concepts. Quality and patient safety are at or near the top of many hospitals’ strategic plans in 2024 and beyond, with many including high reliability as a metric of success. Achieving these goals are possible, but only with the cumulative efforts of data, knowledge, commitment to equity, and action. And yes, the psychology of quality improvement.
Here's to sustainable change and outstanding quality improvement in 2024. Happy New Year
If your team would like to incorporate sustainable quality improvement in your organization, NPIC can support your strategy. Reach out to us to learn more.
